A single oral dose of Calcifediol (25-hydroxyvitamin D) is, for
most people who have not been properly supplementing vitamin D3 for
months, the most important and urgently needed early treatment for
COVID-19
../ To the main page of this site.
Robin Whittle rw@firstpr.com.au 21 December 2021 Twitter: https://twitter.com/RobinWhittle3
(First established 2021-05-02.)
For a comprehensive overview of vitamin
D and the immune system and of the need for proper (e.g. 0.125 mg 5000
IU /day or more, for 70 kg bodyweight) vitamin D3 supplementation,
please see:
https://vitamindstopscovid.info/00-evi/ .
Disclaimer:
You are reading the best efforts of an
electronic technician and computer programmer. What I write
will hopefully help you understand the research, but should not be
mistaken for medical advice. Medical advice is what you get after
a doctor has examined you. Even if I was a doctor, I haven't
examined you!
The recommendation for a
single oral dose of 0.014mg calcifediol per kg body weight (1mg for 55 to 85kg people) comes from
Professor (retired) Sunil Wimalawansa MD, of New Jersey:
LinkedIn (
recommendation). He is a long-time vitamin D researcher:
Google Scholar.
Please read the research carefully and make your own decisions.
If you don't clearly understand it, please consult with someone who
does.
Doctors and nurses can understand all this and evaluate the research,
but they are very busy. Many of them cannot believe that
something so simple and inexpensive as vitamin D could be so crucial to
the proper operation of the immune system, or to ending the COVID-19
pandemic. They should read the research.
Contents
Page
|
Description
|
Last update
|
#guide
|
Guidance for those considering using calcifediol for early treatment of COVID-19.
|
2021-12-21
|
#00-sv
|
Short version.
|
2021-12-21
|
#01-rapid
|
Full version.
#c19vax Sidebar on good 25-hydroxyvitamin D
not being a guarantee of moderate COVID-19 symptoms. To what
extent should the current mRNA and adenovirus vector vaccines be used
with good 25OHD levels and access to multiple early treatments.
The Novavax protein subunit vaccine would be safer, but is not yet
available.
#emergency I am only suggesting a single
oral dose of calcifediol for emergency use. This is not something
where you get sick, order calcifediol and wait days or a week for it to
be delivered. Bolus D3 is the best solution if you don't already
have calcifediol in stock. But since you know of the need for
25-hydroxyvitamin D levels, you and your loved ones will already have
attained this before you get sick - so you won't need calcifediol or
bolus vitamin D3.
|
2021-12-21
|
#02-presc
|
Calcifediol used to be prescription only, and difficult to obtain in most countries.
|
2021-12-21
|
#03-ray
|
Rayaldee is prescription only and is available in the USA for a very high price.
|
2021-12-21
|
#04-faes
|
Faes Farma
in Spain make inexpensive prescription only 0.266m calcifediol capsules
which are available in Spain and Italy and a few nearby
countries. It is possible they might be obtainable without
prescription.
|
2021-11-21
|
#05-fortaro
|
Online, non-prescription
small (0.01mg) tablets in Australia, with delivery of 3 bottles max to
any other country. This is a product of DSM.
|
2021-11-21
|
#06-dvelop
|
Similar non-prescription
tablets available online with delivery to the USA - also from DSM. A similar European product will probably be
available soon.
#liquid how to make 100 of these tablets into a drink or a thicker syrup for ingestion via a spoon or syringe.
|
2021-12-21
|
#07-ratio
| A single oral dose of 0.014mg
calcifediol / kg bodyweight will safely replete any person to 50ng/ml
or more circulating 25-hydroxyvitamin D.
| 2021-12-21
|
#08-lab
|
Lab grade and agricultural grade calcifediol is also available.
|
2021-12-21
|
#99-barc
|
(Low key.) An
observational study of D3 and calcifediol supplementation in Barcelona
is less interesting than it might at first seem.
|
2021-11-21
|
#guide
Guidance - Why you might want to use calcifediol for early treatment of COVID-19, Kawasaki disease etc.:
- Most people who have not been properly supplementing vitamin D3
for months have circulating 25-hydroxyvitamin D (AKA 25OHD) levels of 5 to 25ng/ml (8 to38nmol/L). This is 1/10th to 1/2 of the 50ng/ml 125nmol/L 25-hydroxyvitamin D the immune system needs to function properly. See https://vitamindstopscovid.info/05-mds/ for the most pertinent research on the three vitamin D compounds and the immune system.
- Ordinary healthy D3 supplemental intakes such as 0.125mg 5000IU / day
(70kg bodyweight) take two or so months to raise 25-hydroxyvitamin D
levels from a typical unsupplemented level of 18ng/ml to the desired 50ng/ml or more level needed for
proper immune system function. (Graph below.) This is completely
inadequate for any clinical emergency. So you need either bolus (single, high dose) vitamin D3 (cholecalciferol) or
a single oral dose of ~1mg calcifediol (55 to 85kg bodyweight).
- A small, single oral dose of calcifediol (also known as 25-hydroxyvitamin D, 25OHD, 25(OH)D and "calcidiol")) raises blood vitamin D
(25OHD) within 4 hours to at least this desired, healthy, 50ng/ml 125nmol/L
level. For 70kg 154lb bodyweight, 1 milligram is a good amount. Daily
vitamin D3 should be used to sustain this initially boosted level.
- This is faster than the few days it takes for a bolus dose of vitamin D3 cholecalciferol to raise 25OHD to these
levels, due to the slow conversion of D3 to 25OHD by the liver.
-
All people suffering from COVID-19, sepsis, ARDS, Kawasaki disease, Multisystem Inflammatory Syndrome
etc. urgently need their levels raised to at least 50ng/ml 125nmol/L.
- Calcifediol is now available, in the USA and Australia, without prescription, at affordable prices, in quantities needed for emergency vitamin D repletion: DSM's d.velop and Fortaro.
- If
you already have calcifediol in stock, then for most people,
who have not been supplementing D3 properly for months, a single oral
dose of calcifediol is the most important early treatment for COVID-19
or the other acute medical emergencies listed above in red.
- If you don't already have calcifediol in stock, it is best to use bolus D3
ASAP rather than order calcifediol and wait several days or more for it to to be delivered.
- The best approach is to make such urgent treatments unnecessary
by attaining long-term, lasting, good 25-hydroxyvitamin D levels by
daily to weekly D3 supplementation in the appropriate amounts for your
bodyweight.
- So:
- Use good D3 supplementation now and indefinitely to attain good
25-hydroxyvitamin D levels all year round. (Start with a higher intake
to get your levels up faster.)
- There's no need to buy calcifediol for those in your care who supplement D3 properly.
- If someone else becomes ill and you have no calcifediol in stock, then bolus vitamin D3 is the best option.
- Generally, for long-term vitamin D supplementation, vitamin D3
is perfectly good - there is no need to use calcifediol in the long
term. My only interest in calcifediol is for emergency boosting
of 25-hydroxyvitamin D in clinical emergencies.
Therefore, the only reason for purchasing calcifediol is for for emergency
25-hydroxyvitamin D boosting for other people - friends, family, neighbours (or if you
are a doctor or a nurse, for your patients) - who have not been
supplementing vitamin D properly for a few months, who are reasonably
suspected of or confirmed by PCR test as having contracted COVID-19 (or have sepsis, etc. as mentioned above),
and for whom you want to be ready to boost their 25-hydroxyvitamin D levels in 4
hours, rather than over a few days with bolus D3.
- For a bolus (high, single) dose of vitamin D3 cholecalciferol
I suggest up to 12.5mg 500,000IU D3 all at once, or over two or three
days, for a 70kg 154lb person. Unless they have already got
extremely high 25-hydroxyvitamin D levels there is no chance of
toxicity. (It would take months of unusually high vitamin D3
intakes to reach such levels - such as weeks of 50,000 IU a day or
months or half this - and even then only some people would find this
leads to toxicity - problems with calcium metabolism.)
The person's life hangs in the balance, so you might as well do a proper job.
Bolus D3 quantities as a ratio of bodyweigth. These ratios work
will work for all bodyweights, from newborns to sumo wrestlers: a
single oral dose of 0.175mg 7000 IU per kg bodyweight
for most people, or up to 0.250mg 10,000 IU per kg bodyweight for
those suffering from obesity.
Best give it after a
meal with some fats. Oil-filled capsules may be more effective than
tablets or dry powder capsules. The 2019 ESPEN guideline on clinical nutrition in the intensive care unit
recommends up to 12.5mg 500,000IU D3 in the first week, for an
unspecified but presumably adult bodyweight. See Han et al. 2016 https://aminotheory.com/cv19/#2016-Han
who gave 100,000IU D3 / day for 5 days to mechanically ventilated ICU
patients and so halved the average number of days they remained in
hospital.
- The initially boosted 25-hydroxyvitamin D levels from a single dose of calcifediol or vitamin D3 need to be maintained
in the days, months, years and decades which follow by regular vitamin
D supplements, such as once every day to once a week. Longer
periods between intakes are best avoided.
- For yourself and those in your immediate care, there is no point
in ordering calcifediol in case one or more of you get COVID-19 or any
of the abovementioned diseases. It would be much better for you all to
properly supplement with D3, so you always have good 25-hydroxyvitamin
D levels. Since it takes two months or so of ordinary healthy daily
D3 intakes to attain these levels, you might want to start with much
higher intakes for a week.
- Afshar et al. 2020 https://vitamindstopscovid.info/01-supp/#2020-Afshar found that 70 to 100IU D3 per day per kilogram bodyweight
was a good range of ratios. This was in Dubai, which is sunny but in
which many people - especially women - avoid sun exposure of their
skin. In their use of these ratios with 500 patients over many years,
these doctors found the resulting 25-hydroxyvitamin D levels were
between 40ng/ml 100nmol/L and 79ng/ml 198nmol/L which is a perfectly good range to aim for.
On this basis, with a 72IU/kg ratio, 70kg 154lb gives 0.125mg 5000IU D3 a day.
- If you took 5 times this (0.725mg 25,000IU) per day, for a week,
that would be 4.4mg 175,000IU vitamin D3 in the first week - a modest
bolus dose for an average weight adult to get your level well on its
way to a healthy stable level, in a week rather than a month or so.
#00-sv
Short version
COVID-19 patients urgently need their blood vitamin D levels boosted to 50ng/ml (125nmol/L) or more, within hours
- not days, weeks or months. Only calcifediol - the
pharmaceutical name for 25-hydroxyvitamin D can do this. Calcifediol
is 25-hydroxyvitamin D (25OHD), which
is the form of circulating vitamin D directly needed by all immune system cells. This
50ng/ml or more level is needed for their immune system cells to function properly - to
directly combat the virus and to limit self-harming,
cytokine storm, overly inflammatory responses which cause severe COVID-19. This is only 1 part in 20,000,000 by mass.
For average weight adults (70kg, 154lb) a single oral dose 1.0 milligram calcifediol will do this within 4 hours.
Half this will usually do it too - 1mg is to allow for some
people absorbing it poorly and to allow for some people suffering from
obesity. The excess fat cells in obesity absorb and do not return
both D3 and circulating 25OHD. Obesity is in part an inflammatory
disorder and carries many risks for those who contract COVID-19:
https://aminotheory.com/cv19/obesity/ .
Ordinary, healthy,
vitamin D3 intakes such as 0.125mg (5000 IU) per day (for a 70kg = 154lb adult) will achieve these levels in the long term, but it takes
months.

Bolus D3, such as 3.75mg 150,000IU over three days, as recommended by Dr Lindsey Berkson
https://drlindseyberkson.com/coronavirus-update-integrative-natural-answers/ would probably (depending on absorption, bodyweight and potential obesity) raise levels towards or over
50ng/ml within several days to a week.
This is good, but 1 milligram of oral calcifediol will raise levels towards over
50ng/ml in
4 hours
and so enable the person, in general, to overcome the infection - and
generally to reverse any over-inflammatory responses - much faster.

The original version of this graph is
from the end of the PDF version of this patent by Spanish
pharmaceutical company Faes Farma:
Calcifediol soft capsules
Josep María SUÑÉ NEGRE, Ignacio Ortega Azpitarte, Pepa Del Arenal Barrios, Gonzalo HERNÁNDEZ HERRERO
WIPO WO 2016/124724 Al 2016-08-11
https://patents.google.com/patent/WO2016124724A1/
Most doctors cannot imagine that vitamin D is so important to the
immune system. Most have not heard of
vitamin D based intracrine
and paracrine signaling,
which was first discovered in the mid-2000s
and is not widely enough understood. These needs of the immune
system have nothing to do with the one hormonal function of the vitamin
D compounds - a very low level of circulating 1,25OHD (calcitriol),
produced from circulating 25OHD by the kidneys, which regulates
calcium-bone metabolism.
https://vitamindstopscovid.info/02-intracrine/#02-nothorm .
Calcifediol has been very hard to obtain, but since May 2021, it is
available, without prescription, as a packet of 60 x
0.01mg d.velop tablets =
0.6mg total, initially for USD$30 including shipping, to customers in the USA:
https://dvelopimmunity.com
. In mid-November 2021 the cost is USD$20 a bottle, plus taxes including shipping, within
the USA only. Similar
Fortaro tablets are available from Australia, with shipping of up to 3 bottles (1.8mg total) to any country. Full details below.

#01-rapid
Why RAPID (within a few hours) repletion of circulating 25-hydroxyvitamin D
is a crucial step in preventing or reversing the progression of severe
COVID-19 etc. and why calcifediol tablets or capsules (or potentially
injections or IV drips) are the only way of achieving this
In order to understand the crucial
importance of easily available calcifediol, in the current COVID-19
crisis, and for other deadly health conditions, there are a number of
things you should read, if you have not already done so.
Sidebar on using some other nutrients and Ivermectin as well:
Here we concentrate on vitamin D, but
in the emergency situations described below in which there is an active
viral infection, and/or hyper-inflammatory immune responses, Ivermectin
is likely to be highly effective too. These two
interventions - rapid repletion of circulating 25-hydroxyvitamin D with calcifediol and
anti-viral anti-inflammatory Ivermectin - operate by completely separate mechanisms, and so should
complement each other. Please see:
https://ivmmeta.com and
https://covid19criticalcare.com/ivermectin-in-covid-19/ .
Other nutrients including zinc, magnesium,
boron,
vitamin C and B vitamins (
PMC7428453) should be considered too. Omega 3 fatty
acids are important for immune system functioning, but would take
months to build up good omega 3 levels in the body.
Melatonin is non-prescription in the USA and works well as a COVID-19 early treatment:
https://c19melatonin.com
. Melatonin is recommended by the Front Line Critical Care
Consortium (Dr Paul Marik, Dr Pierre Kory and colleagues):
https://covid19criticalcare.com . Quercetin [
WP] is non-prescription in many countries and can also be used for early treatment:
https://c19quercetin.com .
There is very little vitamin D3 (cholecalciferol) in food. There
is
no such thing as a vitamin D rich food. Unless a person takes
supplemental D3, the D3 they need must be supplied by UV-B
(short-wavelength ultraviolet, ~295nm) light converting 7-dehydrocholesterol in
the skin to D3. This naturally occurs with high elevation
(no more than 45% from the vertical) sunlight, but glass, sunscreen and
clothing block UV-B. There are good reasons to avoid UV-B
skin exposure since it damages DNA and so raises the risk of skin
cancer. Melanin-rich skin greatly reduces the amount of incident
UV-B which reaches deep enough into the skin.
So
people with
black or brown skin have generally low circulating 25-hydroxyvitamin D levels unless they
take proper quantities of supplemental D3, such as, for a 70kg person,
0.125mg (5000IU) D3 a day, on average:
https://vitamindstopscovid.info/01-supp/ . This is especially so if they
are far from the equator and it is winter, or even in summer if they
don't get a
lot of direct sun
exposure. Muslim women are especially at risk if they cover head to toe, even when outside.
Please see the UK white and BAME vitamin D levels by month graph at:
https://aminotheory.com/cv19/#2020-UK-vit-D-BAME
for how low the average levels are in the UK, even for people with
low-melanin (white) skin, in summer. For those with melanin-rich
skin, in summer it is much worse, and marginally worse still - to the
point of being disastrously low - in winter.
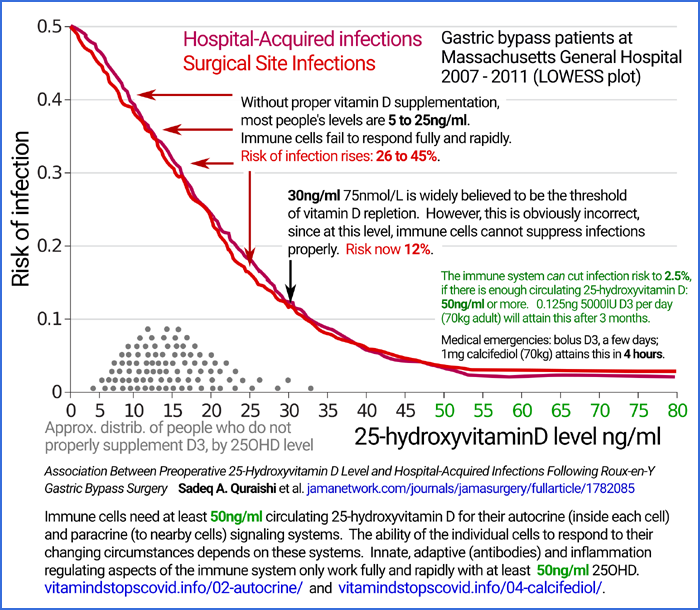
The graph below is from
Quraishi et al. research into hospital acquired
infections and wound site infections from surgery patients in
Massachusetts. It shows clearly that
50g/ml, (50 parts per billion, by mass
125nmol/L)
circulating 25-hydroxyvitamin D (25OHD, calcifediol)
is required for major parts of their immune system to function
properly. In these people, when 25OHD levels were too low,
bacterial and perhaps yeast and fungal infections occurred at much
higher levels than when they had sufficient 25OHD. The affected
parts of the immune system are those cell types which create direct,
innate, responses to bacteria etc. infections and the adaptive
responses - the generation and deployment of antibodies and the
cell-destroying immune cells which get rid of any cell (our own, or bacteria) or virus which antibodies
recognise and attach themselves to.
All these patients were morbidly obese. They were in hospital for a
Roux-en-Y gastric bypass [
WP] operation, which is a major abdominal
procedure. I know of no reason to
believe that their immune cells needed higher circulating levels of
25OHD than is needed by the immune cells of people who are not
suffering from obesity. So this important, and unusually direct,
observation of healthy and unhealthy circulating vitamin D (25OHD =
25-hydroxyvitamin D = calcifediol) levels surely applies to all
people.
Here is
the graph. The article link and summary is at:
https://vitamindstopscovid.info/02-intracrine/#04-quraishi .
This justifies the
40 to 60ng/ml recommendation of the Call to D*Action MDs and researchers in
2008:
https://www.grassrootshealth.net/project/our-scientists/ and more recent review articles such as:
https://doi.org/10.3390/nu12072097 .
Here is another graph, in case anyone needs convincing of how important
good vitamin D levels are to immune function and so to reducing the
chances of severe COVID19. Links to the articles cited are at
https://aminotheory.com/cv19/ .
 #c19vax
#c19vax
Sidebar on to what extent good 25-hydroxyvitamin D levels and
access to multiple early treatments mean it is not necessary to use the
current mRNA or adenovirus vector vaccines
50ng/ml 25-hydroxyvitamin D is
not a
guarantee of having no trouble with COVID-19. I have been
reliably informed of some people who supplemented with 5000 IU vitamin
D3 a day for several months before contracting COVID-19, used
ivermectin and two other early treatments and then all needed to be
hospitalised. It would surely have been worse if their
25-hydroxyvitamin D levels had not been raised in this way, but
COVID-19 is a crapshoot.
I have many reasons for believing that the current mRNA and adenovirus
vector COVID-19 vaccines are not as safe as the public is led to
believe - so they are a crapshoot too. How is one to choose
between the COVID-19 crapshoot - ideally with good 25-hydroxyvitamin D
levels and early treatment such as melatonin, ivermectin, extra zinc,
magnesium, vitamin C, B vitamins, vitamin A (how much?) - and choosing
the vaccine crapshoot to gain significant protection against severe
symptoms? I don't know. People should make their own well
informed decisions and not be pushed into an invasive medical procedure
just because
someone else is worried or insists it is safe and effective.
The COVID-19 crapshoot should not be under-estimated. No matter
how good a person's 25-hydroxyvitamin D levels and no matter what set
of early treatments they can access, I suggest that anyone with serious
co-morbidities - obesity, hypertension, advanced years (how to judge?)
would probably find the non-trivial risks from the current vaccines a
good choice compared to the risks posed by COVID-19.
The
Novavax COVID-19 vaccine
should be a lot safer than the mRNA (Pfizer, Moderna) and adenovirus
vector (Astrazeneca, Johnson & Johnson) vaccines. It
resembles a virus - with 2020 model spike proteins. An adjudavant
causes the immune system to mount a strong response to these spike
proteins. The Novavax vaccine does
not
program our own cells to produce spike proteins, which is the big
problem with the mRNA and adenovirus vector vaccines. The
adenovirus vector vaccines have additional problems due to their use of
a genetically altered chimpanzee adenovirus, which cannot reproduce, to
program our cells. The immune system attacks this, so 2nd and
subsequent doses should be at least partly destroyed if the immune
system is working well. The thrombocytopenia problems of
adenovirus vector vaccines may be due to the adenovirus, not the spike
protein programming of our cells:
Baker et al. 2021.
However, the Novavax vaccine is not available anywhere in December
2021, and the whole question of vaccinating those not already
vaccinated might be moot if the Omicron's current extreme
transmissibility leads most people to being infected anyway, whether or
not they were vaccinated, by the middle of 2022. Being vaccinated
while being infected is not necessarily helpful, and there are no
strong reasons for being vaccinated after infection. I recall
reading that vaccine adverse reactions are higher after infection - and
infection-acquired immunity is so much broader and longer lasting than
vaccine-induced immunity. So I see no reason to vaccinate anyone
who has previously been infected.
There is some vitamin D2 is in some mushrooms and fortified
milk and other foods. These are at low levels and D3 is better in
every respect.
Newly ingested or UV-B produced D3 circulates in the bloodstream. Over a period of days to a week or
so, it is converted by an enzyme in the liver to circulating
25-hydroxyvitamin D.
This is also known as
calcifediol
- and occasionally as "calcidiol" which is a confusing term since it
resembles "calcitriol" (1,25-dihyroxyvitamin D). Hereafter
I refer to it as
25OHD if it is in the body, and as
calcifediol
if it is a pharmaceutical. These are different names for same
molecule. Every microgram of D3 which enters circulation
(the bloodstream) is converted to, very approximately, about 1/3
microgram of 25OHD which goes into circulation. There is no
consensus on the ratio of how many micrograms of D3 are required for
the liver to produce a microgram of circulating 25OHD. 3:1 is a
reasonable estimate, but values of 2 to 6 might be true, depending on the circumstances.
Circulating 25OHD has a half-life of a month or so at healthy levels, such as
50ng/ml (
125 nmol/L).
At higher levels another enzyme, found in many parts of the body, is
more active and breaks the 25OHD down in a self-limiting system, so
the half-life is shorter. Very few people in the whole world are
either getting sufficient UV-B skin exposure all year round or taking
sufficient quantities of supplemental
D3 to have such healthy vitamin D levels.
For
70kg adults, on average,
0.125mg 5000IU D3 a day is sufficient to achieve these healthy 25OHD levels, in most people,
after a few months (see top graph of two, below). See also D3 supplemental intake quantities as ratios of body weight:
https://vitamindstopscovid.info/01-supp/ .
"5000 International Units" may sound like a lot, especially in countries where
most doctors recommend much less, where the largest D3 capsules available are 1000IU, and where
most
doctors are alarmed at anyone taking 4000IU or more. However, it
is a gram every 22 years - and ex-factory, in 1kg lots, pharma-grade D3
costs USD$2.50 a gram
Most people don't supplement properly like this, and for all those who
don't, and who also do not get sufficient UV-B skin exposure all year
round (the elderly get little sun, and their skin is not so good at
producing D3 even if it is exposed . . . and the elderly with brown or
black skin . . . . . ) and so have levels in the 5 to 25ng/ml range
most of the year. At these lower levels circulating
25OHD's half life is, very approximately, two months or so.
Circulating (meaning in the blood, specifically in the liquid = plasma part
of the blood, rather than the cells) 25OHD is what is
measured in
vitamin D blood tests.
Circulating 25OHD diffuses into the tissues and into cells, through
their cell membrane. There is no active transporter system to get it into cells.
This 25OHD which diffuses from the blood into cells is required by many
types of cells for their intracrine and paracrine signaling systems,
where it is consumed, and turned into
1,25OHD
AKA calcitriol inside the cell. This is part of a signaling
system - conveying information within each cell, from the mechanisms
which detect a particular external circumstance to the mechanisms in
the nucleus which control which genes are transcribed into messenger
RNA molecules. The mRNA molecules control how much of each type
of protein the cells make. So changing how genes are copied into
mRNA molecules changes the behaviour of the cell.
Neither vitamin D3 nor 25OHD is a hormone. A hormone is a substance
which is produced in one location in the body and travels through
the bloodstream and by diffusion in the tissues to cells in distant
parts of the body. The level (the chemical concentration, such as
in trillionths of a gram per gram of blood) affects those distant cells
by controlling some aspects of the cell's behaviour in proportion
to the concentration of the hormone molecules. Hormones are
long distance cell-to-cell signaling molecules of endocrine (hormonal)
signaling system.
Circulating 25OHD has two roles. The first one is known by all
doctors and nurses. The second role is hardly known at all.
Most
doctors have a vague idea of "vitamin D" affecting
immune cells and cells of other types, which is true. However, very few doctors understand the mechanisms -
intracrine and paracrine signaling - since these have mainly been discovered since the mid-2000s.
https://vitamindstopscovid.info/02-intracrine/
The
first role of circulating 25OHD
is to provide the
kidneys with a small amount of 25OHD which they
convert (in a process controlled by the parathyroid hormone, the level
of which is controlled by various aspects of the body's calcium handling
system) into 1,25OHD (calcitriol) which goes into
circulation. This
circulating 1,25OHD acts as a hormone.
The exact level of circulating, hormonal, 1,25OHD is precisely
controlled by the kidneys. This level is sensed by multiple types
of cells in various parts of the body and controls both the absorption
of calcium from the intestines into the bloodstream and the actions of
osteoblasts, osteoclasts and other cells which are involved in the
constant remodeling necessary for
bone health. The calcium level in the blood need to be very tightly regulated, since it affects numerous processes in all cells.
Unfortunately it is common for even the most experienced
vitamin D researchers to state that "vitamin D" (here meaning the three
compounds collectively - D3, 25OHD and 1,25OHD) "is a hormone", or "is
a
secosteroid
hormone" which
sounds even more impressive. The vitamin D compounds are
extraordinarily important, but the only one of them which acts as a
hormone is 1,25OHD, and this is only when it is circulating in the
bloodstream, which it does at a very low level, such as 0.045ng/ml .
Sidebar on 1,25OHD:
1,25OHD is the only one of the three vitamin D compounds which strongly activates
vitamin D receptor (VDR) molecules. A 1,25OHD molecule binds to a VDR molecule and together, as a bound complex, they alter the
patterns of gene expression (copying of gene data in the DNA to
messenger RNA) and so the rates at which the cell produces various
proteins. (You may see 1,25OHD referred to as "activated vitamin
D". Vitamin D terminology is confused and
confusing.) The changes to gene expression depend entirely
on the cell type.
The "Vitamin D Receptor" should ideally be known as the "Calcitriol
Receptor" or the "25-hydroxyvitamin D Receptor". It is not
activated to any significant degree by either vitamin D3 or
25-hydroxyvitamin D.
In any given cell type, VDR molecules can be "activated" (bind a
1,25OHD molecule, and so change their shape and behavior) when any of these three processes occur:
- Hormonal signaling: circulating 1,25OHD diffuses into the cell
and binds to VDR molecules in the cytosol (the main volume of the cell,
not the nucleus).
- Intracrine
signaling: 1,25OHD molecules just produced in the cytosol binds to VDR
molecules in this cytosol - all within the same cell.
- Paracrine
signaling: 1,25OHD produced as part of intracrine
signaling in nearby cells, diffuses from
that cell into a nearby cell and binds binds to VDR molecules in that
cell's cytosol. (The nearby cell is probably of a different type
to that which produced the 1,25OHD.)
In all cases the bound complexes of 1,25OHD and VDR "migrate" to the nucleus.
(I
have not found a good description of this. Perhaps they simply
diffuse. I haven't read of an active transporter system to push
them into the nucleus, and as far as I know, the bound complexes don't
have a GPS and propellers so they actually move themselves towards and
into the nucleus.)
Once in the nucleus, the activated VDR molecule binds to a retinoid X
molecule and the resulting trimer complex interacts with various DNA
management
arrangements, the details of which vary from one cell type to the next,
including how parts of particular chromosomes are unwound
from their normally tightly wound state (not the spiral structure, see
histones) to expose particular genes to the enzymes which copy their data
to new messenger RNA molecules, which go to the cytoplasm and direct
ribosomes [
WP] to make a particular protein.
So the presence of 1,25OHD-VDR complexes in the nucleus alters the
cell's behavior by altering its protein production by altering its
transcription of genes. Exactly which genes are upregulated and
downregulated differs from one cell type to the next.
This circulating, hormonal, 1,25OHD is at a very low level: such as
1000 times less concentrated than the (ideally) 50 parts per
billion
of 25OHD.
https://vitamindstopscovid.info/02-intracrine/#02-nothorm Its half-life is a day or less. The kidneys can
maintain the required level pretty well with circulating 25OHD levels
of 20ng/ml or so - though, unfortunately, many people don't even have
this. Some people have 25OHD levels below 10ng ml, and so have
poor bone health. Doctors generally think of deficiency
being below 20ng/ml or perhaps 30ng/ml (75nmol/L) - but
this is just for bone health.
The
second role of circulating 25OHD is the one everyone needs to
understand, since it concerns all aspects of the immune system, as well
as a large number of other cell types which have not yet been so well
researched.
Very few MDs understand this.
In this role, circulating 25OHD is used by
numerous cell types, all over the body, to be converted
inside the cell to 1,25OHD, for the purpose of activating vitamin D receptors
inside the cell, to alter gene expression and so protein synthesis and the whole operation of
that particular cell. This is
intracrine signaling
- a form of
signaling which occurs entirely within the
cell.
Other types of molecules are involved in other intracrine signaling arrangements and here we are only interested in
25OHD being converted to 1,25OHD. This intracrine signaling
is not to maintain a steady state, such as with calcium- bone or some
other stable bodily system. The intracrine signaling conversion to
1,25OHD is only turned on in particular circumstances. Vitamin
D based intracrine signaling is a crucial part of how most immune cell
types, and many other cell types,
respond to their changing circumstances.
This has nothing to do with hormonal signaling. The levels
of 1,25OHD produced inside the cell are much higher than the very low
levels of hormonal circulating 1,25OHD. The half-life of
1,25OHD inside the cell is short - probably hours or less - since
enzymes there degrade it.
Paracrine signaling is a
closely related signaling system in which 1,25OHD, produced in a cell
from 25OHD - as for, or as part of, intracrine signaling - diffuses out
of the cell and to nearby (millimetres) cells,
which sense its level and alter their behavior accordingly.
Since I couldn't find a good, illustrated,
tutorial on intracrine and paracrine signaling, I made this page:
adapting illustrations from a 2011 article by Martin Hewison and
colleagues, in which they report their discoveries. If you
have time,
please read this page and at least some parts of the research articles it cites.
If you have understood the current page so far, you know more about
vitamin D intracrine and paracrine signaling than the great majority of
doctors. By reading and understanding the 02-intracrine page, you
will attain a still better understanding of these processes.
It includes references to research which:
- Indicates that 50ng/ml
or more circulating 25OHD is needed for immune cell intracrine and
paracrine signaling to work properly - at least for those cell types
which directly defend against bacteria. (Quraishi et al. 2014. See the graph above.)
It is reasonable to assume from this, and from observations of vitamin
D levels which reduce excessive inflammation, that Th1 regulatory
lymphocytes need similar circulating 25OHD levels to function properly.
- Shows in full detail how Th1 lymphocytes rely on good levels of
circulating 25OHD for their intracrine signaling. (Chauss et al. 2021.) When 25OHD
levels are very low, Th1 lymphocytes remain stuck in their initial
pro-inflammatory program and fail to respond to signals which should
cause them to switch to their anti-inflammatory shutdown program. This
continued excessive inflammation (cell-destroying immune responses) is
the cytokine storm which
causes some people to develop severe COVID-19.
It
is reasonable
to assume that the exact same dysfunction - Th1 dysregulation of
self-destructive inflammatory immune responses, due to inadequate
vitamin D levels (circulating 25OHD), together with similar failures of
intracrine/paracrine signaling by other regulatory cells - is the
primary cause of sepsis
[Wikipedia link: WP], Kawasaki disease [WP and https://aminotheory.com/cv19/#2015-Stagi], Multisystem Inflammatory Disorder [WP] and ARDS [WP] - however see the note below on helminths.
I regard this work: Chauss et al. 2021 (linked to, summarised and discussed at: https://aminotheory.com/cv19/icu/#2021-Chauss) as the most important research work ever done on the mechanisms of severe COVID-19. Every doctor should understand this, but the research is relatively new and so it is not yet widely known.
- Report on the remarkable effectiveness of a small (0.532 milligram), single, oral dose of calcifediol, which goes into circulation within hours, where we call it 25OHD, raising initially low levels to healthy 60ng/ml
or more, on average, within a few hours. This is the work
of Castillo at al. 2020 (linked to and summarised at: https://aminotheory.com/cv19/#2020-Castillo), in Cordoba, Spain and is well known among all
vitamin D researchers and vitamin D aware doctors and
nurses.
This single dose of 0.532mg calcifediol, given at the earliest opportunity to hospitalised COVID-19 patients is the main reason why ICU rates were reduced from 50% to 2% and deaths from 8% to zero.
This is extraordinary result is partly due to the control group having
a greater incidence of co-morbidities, but the impact of the
calcifediol treatment is still responsible for most of the reduction in
ICU admissions. (The reduction in deaths is not so statistically
significant due to the small number of subjects in the trial.)
A single dose of calcifediol such as this would be still more effective
if given withing a day or so of COVID-19 infection being known, such as
from a positive PCR test. The Castillo trial involved giving the
dose at a much later stage - when the person's symptoms were serious
enough that they were admitted to hospital.
Once you understand vitamin D intracrine / paracrine signaling, the need for
50ng/ml
or more circulating 25OHD for it to work properly, that many types of
immune cell need such levels to work properly (those cell types which directly attack
pathogens, develop antibodies and correctly regulate potentially
self-destructive inflammatory immune responses - Chauss et al. 2021), then it is clear why
low 25-hydroxyvitamin D (25OHD = calcifediol) drives the development of severe COVID-19 and why a tiny
quantity of oral calcifediol is so extraordinarily effective at preventing
hospitalised COVID-19 patients from progressing to full-blown severe,
cytokine storm, endothelial cell destruction, hypercoagulative blood,
micro-embolisms and larger blood clots,
severe COVID-19.
If you are keen, you will find links to and summaries of dozens of research article here at
https://vitamindstopscovid.info and at its more extensive and less well organised companion
https://aminotheory.com/cv19/ . Please also see
https://VitaminDWiki.com and the meta-analysis of the latest vitamin D intervention and observational studies concerning COVID-19:
https://vdmeta.com
.
Those with the most inquiring minds will want to
know why humans, domestic animals and agricultural animals suffer,
generally and according to considerable genetic variation, from
such a large number of overly-inflammatory conditions. The answer
is that we have no longer are infested by
helminths (intestinal worms):
https://vitamindstopscovid.info/06-adv/#02-helminths .
There are a plethora of reasons why everyone should supplement vitamin D3 to aim for 25OHD levels of
50ng/ml
or so. For suggestions for how much D3 to take, on average
(it is generally regarded as OK to have larger intakes up to a week
apart), depending on body weight and morphology (people suffering from obesity need
more D3 per kg bodyweight), please see:
Long-term supplementation along these lines raises circulating 25OHD
over a week or two, and then over a few months, to a final healthy
steady state, all year round.
For most people, this is fine and there is no need for them to think about calcifediol == 25OHD.
#emergency
However, if a person is suffering from, or at significant risk of developing, any of these conditions:
- Severe COVID-19 - or probably any symptomatic form of COVID-19,
since this carries high risks of lasting harm, even if the person does
not die.
- Sepsis
- infection triggers gross immune system dysregulation with
inflammatory (cell destroying) processes wreaking havoc all over the
body - especially the lungs.
Sepsis develops rapidly, has a variety of mixed up symptoms, is
frequently not diagnosed anywhere near fast
enough and can kill within hours. [WP] See also Reyes et al. 2021 who state that Bacterial sepsis and severe COVID-19 share similar clinical manifestations. According to Rudd et al. 2020 nearly 20% of all deaths, worldwide, are due to sepsis.
- Kawasaki disease - triggered in children, especially by COVID-19,
including with very mild COVID-19 symptoms. KD - like sepsis,
MIS, ARDS and severe COVID-19 - is a condition of extreme, overly
inflammatory, immune system dysregulation. It is primarily a disease of the vasculature - blood vessels. [WP]
- Multisystem Inflammatory Syndrome (MIS). [WP] AKA Paediatric
Inflammatory Multisystem Syndrome Temporally associated with Severe
acute respiratory syndrome coronavirus 2 (PIMS-TS) Darren et al. 2021: https://doi.org/10.1017/S0007114521001562
report on melanin rich skin UK children in ICU with this condition
averaging 7.8ng/ml 25OHD. MIS-C and Kawasaki disease are separate
diagnostic categories which cover parts of a spectrum of disease with
the same underlying causes, but with somewhat different symptoms.
- Acute Respiratory Distress Syndrome (ARDS). [WP]
- Pre-eclampsia [WP] From Borzychowski et al. 2006 "Pre-eclampsia
is a common and potentially dangerous disorder of human pregnancy. The
maternal syndrome of hypertension, proteinuria and oedema is part of a
severe systemic
inflammatory response that includes leukocyte and endothelial cell activation."
There are plenty of research articles on pre-eclampsia and vitamin D,
but this does not mean that most OB/GYNs recognise this and so ensure
that pregnant women have good 25-hydroxyvitamin D levels.
then it is likely that their circulating 25OHD
levels are dangerously low and have been for weeks or months. (Also, these infections can
marginally reduce these levels, presumably due to
25OHD being consumed by immune cells' intracrine and paracrine signaling
systems.)
Without rapid repletion of their 25OHD, they will be at high risk
of serious harm and death
- depending on the success of any
anti-inflammatory drugs, which MDs and nurses frequently use at present to
tackle these emergencies. MDs and nurses also tackle other
problems such
as high or low blood pressure. These anti-inflammatory drugs -
such as prednisone and dexamethasone can cause psychosis and deadly
fungal diseases. See:
https://vitamindstopscovid.info/05-mds/#04-cortico . They also
reduce innate and adaptive responses to bacteria, viruses and fungi.
Bolus (AKA
stoss or
loading dose) D3, as described above, usually helps. But these
people need their 25OHD levels raised
now, not in days or a week or so.
Such brief, higher than normal, D3 intakes, or the ~1mg single dose oral calcifediol discussed below - are unlikely to
cause any harm, even if someone has been supplementing higher than
ideal D3 levels for months. So there's
no need for a 25OHD blood
test, unless perhaps the results can be known in a few minutes.
Time is of the essence and the sooner their 25OHD level is raised the
better chance the person has of overcoming any pathogens and what might
otherwise be a progression to self-harming hyper-inflammatory
immune system dysregulation.
#02-presc
Calcifediol is a magic bullet, but until early 2021, has been
prescription-only and very hard to obtain except in Spain, Italy and
some nearby countries.
Magic bullet
AKA
silver bullet
is a strong term in medicine. It broadly refers to a drug
which knows exactly where to go in the body, and what to do there, to
completely fix a particular problem.
However,
calcifediol is not a drug. It is simply the molecule the
immune system needs to function. It doesn't go any one place - it goes
into solution in the blood stream and then diffuses into all
tissues. There it diffuses into most or all cell types. All
immune cells - and many other types of cell - need it inside their cell
bodies so it can be used when their vitamin D based intracrine signaling systems are
activated. So it does go exactly where it is needed - into
circulation and from there into all the tissues and cells.
I am just an electronic
technician, and you should make up your own minds about all this, after
reading the research yourself, rather than rely on my opinions.
However, I think it is reasonable to regard a milligram or so of
calcifediol (for 70k bodyweight), in a one-off oral dose (with continuing support with D3 in the
days which follow), as a
magic bullet
when tackling the conditions listed above, all of which are made very
much worse by low circulating 25OHD levels. Most
likely if the person had good vitamin D levels of
50ng/ml or so, they would not have become ill in the first place.
0.532mg of oral calcifediol (in oil-filled capsules, which improves
absorption from the intestine into the bloodstream) provided dramatic
benefits to the hospitalised COVID-19 patients in Cordoba (Castillo et
al., above).
The purpose of the rest of this page is to discuss how such single dose calcifediol treatments can do much the same
magic bullet
work as in Cordoba, in the abovementioned
#emergency emergency medical conditions,
where the primary, correctable, problem is low circulating (blood) levels of 25OHD = 25-hydroxyvitamin D = calcifediol. The earlier they can have their level boosted, the better.
Assuming the person is conscious and can ingest liquids, all we need to
do, for 70kg bodyweight is give them about 1mg oral
calcifediol and we will have
their 25OHD levels high enough to meet the needs of all their immune
cells, within a few hours. (In principle injections or IV drips
could be used as well, but this page concerns only oral calcifediol.)
The precise amount is not critical. 0.014mg calcifediol per kilogram bodyweight is
recommended by Prof. Sunil Wimalawansa, which is about 1mg for 70kg.
#03-ray
Rayaldee from the USA
In the middle of 2020, calcifediol was difficult to
obtain. As far as I know, the only option in the USA (and
perhaps Canada) was the
prescription capsules "Rayaldee". As detailed at
https://aminotheory.com/cv19/#calcifediol-availability
a packet of Rayaldee contains 30 capsules, each containing 30
micrograms = 0.03mg of calcifediol. The whole packet contains 0.9mg of calcifediol. Since each packet costs
USD$1,206.88, this is
USD$1,340.98 per milligram.
Rayaldee uses a patented sustained release arrangement. This
supposedly confers benefits for the patients for which it is FDA
approved in the USA, such as those with kidney disease. However,
it makes no sense that this sustained release provides benefits in
addition to those which arise from the calcifediol being quickly
absorbed in the intestine, since the half-life of calcifediol in the
blood is weeks at least, and more likely one or several months.
I believe that Rayaldee is a vastly overpriced preparation and that its
promotion inherently disparages the value of plain oral
calcifediol. However, my opinion is of no consequence regarding
anyone's treatment decisions. Ask your doctor what he or she
thinks - and point them to this page.
Hidroferol from Spain and Neodidro from Italy
Until early 2021, to the best of my knowledge, the only other source of
pharma-grade calcifediol ready for oral use in patients was the oil-filled
capsules and glass ampoule forms of
Hidroferol, the awkward trade name of long-established Spanish company
Faes Farma. More details at:
https://aminotheory.com/cv19/#hidroferol .
However, in May 2021, I was told of
Italian Neodidro, which are very
similar or perhaps identical capsules, also prescription only, which
are available for €10 for 10 capsules of 0.266mg each. This is
about USD$12.14 and so
USD$4.56 per milligram. More details at:
https://aminotheory.com/cv19/#neodidro
. Someone on Twitter mentioned that his sister in Italy asked
for some Neodidro at a pharmacy and had to wait for it to come back into stock - but
that she would be able to obtain it without a prescription. Can
anyone tell me more about an such non-prescription sources of
calcifediol?
These
Hidroferol capsules, each containing
0.266mg calcifediol,
were used in the Cordoba trial
https://aminotheory.com/cv19/#2020-Castillo, so we know these are good. The
patients received two such capsules at the earliest opportunity, and
then one capsule on days 3, 7, 14, 21 etc. The first
two capsules made all the difference. The subsequent
smaller doses would have maintained the newly boosted circulating 25OHD
levels perfectly well,
but regular vitamin D3 capsules, averaging (for 70kg adults) 0.125mg
5000 IU per day (
https://vitamindstopscovid.info/01-supp/), would have maintained these levels just
as well.

As far as I know these are available within Spain. They seem to be available from
pharmacies in Georgia (the country, not the US state). The 43.71 Gel price for ten capsules equates to about USD$14.
If we assume a price of USD$15, for 10 x 0.266 = 2.66mg, then this is
USD$5.64 per milligram. The challenges are having a prescription for it, finding a seller who
will export it to the country of interest, and getting it through
customs.
#05-fortaro
DSM's Fortaro, for customers in Australia - and now to any other country
In February 2021, leading Dutch human and
animal feed supplement manufacturer DSM (
https://dsm.com ,
WP) launched
Fortaro with online
sales, no prescription required, for customers in Australia. I
bought some and you can read all about it at:
Each bottle costs AUD$24.99 (about USD$19.22 and contains
60 small (150mg)
tablets, each with 10ug
0.01mg calcifediol per tablet.
By May 2021 they had updated their system to handle free shipping to any country,
with a maximum of 3 bottles (
1.8mg calcifediol) per international
order. (Shipping is free to Australian destinations, and there is no 3 bottle limit.)
The cost of 3 bottles (1.8mg calcifediol) was AUD$74.97, which (2021-06-12) after adding 6% for credit card fees and
exchange rate spread, is about USD$61.20. Assuming no entry
fees to the USA, which seems reasonable, this is
USD$34.00 per milligram calcifediol. However, the quantities are limited to 3 bottles
per order to overseas destinations. Delivery to the USA or Canada
would take a lot longer
than ordering from the USA.
#06-dvelop
DSM's d.velop for customers in Canada and the USA
In April 2021 DSM launched a
similar product
d.velop for online sales, with no prescription required, for
customers in the USA and Canada:
However, within a few months the shipping was only to addresses in the
USA. By November 2021, the price was reduced from USD$30 for 60
0.01mg tablets to USD$20. (The default pricing of $18 is for a
continuing "subscription" of 3 bottles every 3 months.)
Since:
- There are numerous packet forwarding companies in the USA - such as the one I use: https://www.shipito.com
- who can either purchase items from sellers or ship packages to you in
other countries if you buy them directly with delivery to their
warehouse.
- The product is labeled as "Vitamin D", is made in Switzerland and is non-prescription in the USA, so I expect there would be few
difficulties getting these into other countries.
people in
countries other than the USA and Australia
have choices such as these for obtaining either of these
packets/bottles of 60 x 0.01mg calcifediol tablets:
- Order up to 3 Fortaro tablets from Australia. Maybe make repeat orders to the same or different addresses if more are required.
- Find a packet forwarding company in Australia and order more than
3 bottles of Fortaro, to be sent to the company - or have the company order them -
and then have the company ship them to any other country.
- This is probably the best option: Find one of the numerous packet forwarding companies, such as https://www.shipito.com/en/ in the USA and get them to send d.velop tablets, again perhaps with them placing the order.
So I believe that these 60 x 0.01mg calcifediol tablets are available, in practical terms, to anyone
who wants them, no matter which country they live in.
Here are the details of the
d.velop tablets:
Each packet contains 60 tablets each with 10ug 0.01mg calcifediol. This is 0.6mg calcifediol for USD$20 including shipping within the USA. So this is USD$33.33 per milligram calcifediol. However,
when I tried ordering some in November 2021 for delivery to ShipiTo in
California, each USD$20 bottle had an additional USD1.90 tax added.
In May 2021 I ordered 3 packets, which were sent to ShipiTo.com in
California, who posted the package to me using USPS. (Their
cheapest shipping option uses AusPost, who apparently won't handle
packages containing nutritional supplements. Overall, with their
handling costs, this adds a lot to the cost.) The package arrived on
2021-05-21.
These tablets are almost identical to the Fortaro tablets. They
are 148mg, 6mm in diameter and 3.5mm high. Like the Fortaro
tablets they disintegrate rapidly in water and, for me at least, have
no taste. They contain the same 0.01mg quantity of
calcifediol. Instead of being in a plastic bottle, they are
in a small box with 6 blister pack trays of 10 tablets each. They
are the "product of Switzerland" and the bar code is 810077300008.

The benefit of calcifediol over D3 is very fast repletion. So
calcifediol is only really needed for emergencies.
Therefore, it needs to be ordered and ready to use when the emergency
occurs - such as someone who has not been robustly supplementing
D3 for few months is diagnosed with COVID-19, sepsis, Kawasaki disease
etc.
In July 2021, DSM received approval for similar products in Europe:
https://efsa.onlinelibrary.wiley.com/doi/10.2903/j.efsa.2021.6660 .
#liquid
Making a drinkable suspension from these 0.01mg calcifediol tablets - or a spoonable syrup with water and glycerol
For many people, to ingest 1mg of calcifediol, it will be a little odd,
but perfectly practical and not at all unpleasant to swallow 3 or maybe
a few more of these tablets, take a sip of water, swallow and repeat 33
times or so.
However, there may be problems taking larger numbers of tablets like
this - or even taking tablets at all for babies and toddlers.
Also, in a medical setting, some patients might think the doctor or
nurse is giving them an excessive quantity of something if it
requires 100 tablets or so.
The alternative is to mix the tablets into some water and make a
drinkable suspension / slurry. On 20 December 2021 I tried this out
with
100 d.velop tablets =
1mg. I think the Fortaro tablets would behave in exactly the same
way. I used a small (150ml) glass. Please click
the small image to see a larger version. The USB plug is an
everyday item so you can perceive the size of the small tablets and
small glass.
The tablets occupy a volume of about 20ml. The tablets start
puffing up within seconds when water is added. This is not a fizzy
reaction - they gently disintegrate as they absorb water.
I added 50ml of cold water. After two minutes or so the tablets puffed up:
I stirred this and it formed a suspension, which settled to some extent
after a minute or two. The top 8mm or so of water has
fewer suspended particles.
After taking the third photo, I stirred it and drank it. A little was left in the glass, so I added some more water.
Stirring seconds before drinking is important, since it does
settle. There's no taste. I guess it would be similar to
drinking a solution of chalk, though not as heavy as actual
chalk. There are 14.8 grams of tablet and 50 grams of water, so
this is a 23% by mass suspension / slurry.
I don't know of any professional pharmaceutical preparations which
directly resemble this, but a 5% suspension of cephlahexin is somewhat
similar.
I think that by adding some
glycerol - maybe 15ml glycerol and 35m; water, or greater quantities of
both - that the mixture would be more viscous and so hold the particles
in genuine suspension for longer. A pharmacist might be able to
suggest something better. This cephlahexin suspension contains sodium lauryl sulphate, methylcellulose 15, dimeticone [WP],
xanthan gum, and pregelatinised starch. However, I don't think
there is a need to go to so much trouble with a medication which only
needs to be taken once. Probably some fruit syrup would be
helpful with children.
To explore making a
thicker suspension, I tried a single Fortaro tablet with a little
glycerol.
It remained firm, except at the edges. I added a little water and
after a minute or two the tablet puffed up and then disintegrated when
I pressed it with a spoon. This is probably a
better approach than the water suspension technique above. I suggest, but have not tried with multiple tablets:
Count out the tablets. Number of tablets = bodyweight in kilograms x 1.4. Each tablet occupies about 0.2ml of space.
Make a 50/50 water/glycerol mixture and add about the same volume of this as the volume taken up by the tablets.
Wait a few minutes, crush and stir.
I believe this would be suitable for ingestion via a spoon or syringe
for any conscious person including babies. It is sweet and
syrupy, with fine grains of suspended tablet particles.
I am 69kg and take 1.25mg 50,000 IU vitamin D3 a week (7143 IU /
day). I guess my 25-hydroxyvitamin D level is most likely to be
in the 60 to 100ng/ml. I could not be anywhere near potentially
toxic levels (above 150ng/ml) and I have no concerns about this
single
1mg calcifediol dose causing toxicity. (I formed this opinion
after consulting with Prof. Wimalawansa, who has decades of clinical and
research experience with vitamin D compounds.) In terms of
long-term capacity to raise 25-hydroxyvitamin D levels, this 1mg
calcifediol is probably equivalent to 3 or 4mg vitamin D3 = 120,000 or
160,000 IU, which is a small bolus dose.
#07-ratio
How much calcifediol to use, as a ratio of bodyweight?
In this emergency vitamin D repletion
scenario, you would be using
Fortaro and
d.velop products quite differently to the
daily (or twice daily for
d.velop) use the manufacturer
recommends. So you would be taking
full responsibility for
our actions - not giving me or DSM a hard time if something bad happens.
The prescription-only 0.266mg
Hidroferol and
Neodidro were probably initially intended for long-term supplementation, and so
for a capsule to be taken every week or few weeks. However, I
understand that Faes Farma provided the Hidroferol capsules for the
Cordoba trials, so I doubt they would quarrel with anyone using them
two at a time (or perhaps four at a time) to save people from
suffering, harm and death due to severe COVID-19.
Assuming plenty of calcifediol is available, I tried to arrive at a
micrograms per kg bodyweight ratio, which would be helpful for
everyone, from babies to sumo wrestlers. I consulted with
Prof.
Sunil Wimalawansa MD, of New Jersey (long-time vitamin D researcher
CV,
Google Scholar) he advised that
14 micograms per kg bodyweight would be a good ratio to use.
This is confirmed in a
post Oral Calcifediol Repletes Blood Vitamin D Concentration within 4 Hours on Dr Wimalawansa's LinkedIn feed, where he has (2021-11-20) 13,143 followers.
This is about double the micograms / kg bodyweight which was so
successful in the Cordoba trial and is 1mg for a 70kg
person.
Doubling the amount per kg gives some allowance for
poor absorption and people suffering from obesity, for whom it is more
difficult to raise their circulating 25OHD levels due to excessive fat
absorption.
https://aminotheory.com/cv19/obesity/
1mg of calcifediol is very approximately as effective, in long-term
use, for raising circulating 25OHD levels, as 3 times this amount of
D3. (On this basis, 1mg calcifediol is roughly equivalent to 3mg 120,000 IU
vitamin D3 cholecalciferol. This is would be a small bolus
D3 dose, and on average the Cordoba
https://aminotheory.com/cv19/#2020-Castillo patients did well with a little more than half half this.
Since this is a single dose, there is no risk of toxicity unless
perhaps the person had been excessively supplementing D3 for
months.
Due to the urgency of the situation, with the person's long-term health
and perhaps life hanging in the balance, it makes sense to do a good job of repleting
circulating 25OHD levels in a way which will still be effective if
obesity and/or marginally poor absorption are problems.
So a 70kg person would get 1.0 mg = 100 tablets of
Fortaro (100 / 60) * 25 =
AUD$41.67 or
d.velop tablets at a cost of (100 / 60) * 30
USD$33.33. This is a good deal considering how serious all the above conditions
could be. Even if it made only a barely perceptible difference of
a few percent to the outcomes, it would be a good deal.
In
Cordoba
https://aminotheory.com/cv19/#2020-Castillo, with presumably some or many of the patients suffering from
obesity, and so with bodyweights well over 70kg, 0.532mg calcifediol (54
d.velop tablets costing
USD$27) was the primary cause of the
huge reduction in symptoms, suffering and need for
intensive care.
If the Cordoba patients averaged 76kg bodyweight (this seems
reasonable, though no such data is presented) then in this trial the
crucial initial dose of calcifediol would have been about 0.007mg per kg bodyweight.
If the calcifediol was available on only limited quantities, I suggest
distributing it evenly over multiple people according to their bodyweight
and risk of serious harm. Any amount will
help.
0.014mg calcifediol per kg bodyweight is an approximate recommendation, not some critical ratio to be adhered to closely. It would be fine to remember:
55 to 85kg: 1mg calcifediol
86 to 119kg: 1.5mg calcifediol
120 to 190kg: 2mg calcifediol
which covers most adults and older adolescents. For babies and
children, the frail, overweight and obese adults outside this range,
0.014mg / kg is good guidance.
Another way of thinking about it, with
Fortaro or
d.velop 0.01mg tablets is:
Multiply the bodyweight in kg by 1.4 to get the number of tablets.
Please see this section, which I wrote before these two DSM
product releases. I suggest a
single calcifediol dose followed by
robust D3 supplementation in the days, weeks and years which follow:
I suggest taking D3 and perhaps calcifediol with some oil, such as
fish oil, or
at least towards the end of a substantial meal which contains fat, to
activate the fat absorption mechanisms in the upper
intestines. Don't wash it down with a lot of water or any
other drink. However, while D3 is more soluble in fat than
water, calcifediol, with its extra hydroxyl group, is more soluble in
water.
Please remember that you are reading the
best efforts of an electronic technician - not a doctor!
However, this proposal is based on the recommendation of one of the
foremost vitamin D researchers who is a retired (but still very active)
professor of medicine.
My interest in these
Fortaro and
d.velop tablets is to use several
dozen to two hundred or so of them at once, which is completely different to how these
products are intended to be used. If you do this, it
your decision.
There are a few things to remember about these excellent DSM products -
and of Hidroferol and Neodidro:
- Despite the claims of DSM that Fortaro and d.velop have
advantages over vitamin D3 cholecalciferol for long-term
supplementation, I see no reason to
believe this - unless it could somehow be shown that particular
individuals had significant absorption problems for D3 and/or liver
conversion problems, with no such absorption problems for
calcifediol. This may be the case:
- While these calcifediol tablets and capsules would work for
long-term supplementation, they are a lot more expensive than
alternatives such as 100 1.25mg 50,000 IU capsules for USD$30.
(Link to US manufacturer deleted at their request due to concerns about
US regulations regarding advertising COVID-19 treatments.) My
wife Tina and I take one a week - so 0.179mg 7143IU a
day.) USD$30 buys 125mg D3 = USD$0.24 per milligram
D3. For USD$20, 60
d.velop tablets provide a total of 0.6mg calcifediol. Assuming we
accept the 3:1 ratio suggested by DSM, this is equivalent to only 1.8mg
D3. This is USD$11.11 per 1mg D3 equivalent. On this basis,
for long-term nutrition, d.velop is 46 times as expensive than these
50,000IU
D3 capsules.
- The
only reason I am interested in these products is for one-off
emergency vitamin D repletion. This means they must be purchased
ahead of time in anticipation of someone becoming ill with
one of the
abovementioned conditions, with that person not having been
supplementing vitamin D3 properly for several months beforehand, and so
reasonably assumed to have 25-hydroxyvitamin D levels far below the
desired 50ng/ml 125nmol/L.
- Most doctors know little or nothing about all the research
mentioned on this page, so they might be opposed to the suggestions
here. Please ask them to read this page and hopefully at least look
a the research articles cited here. Another account of what they need to know, with more references, is at https://vitamindstopscovid.info/05-mds/ .
#08-lab
Lab grade and agricultural calcifediol
Lab grade calcifediol is also
available but MDs would probably have to break regulations and so
threaten their career of they did not use pharma grade - though with
these tiny quantities, the lab grade calcifediol would be just as
effective and with no possibility of there being a significant quantity of
impurities.
Likewise, almost certainly, the much cheaper
agricultural feed products I researched at:
https://aminotheory.com/cv19/agri25OHD/ where a bucket of poultry water feed powder costs about USD$100 and contains 1.875 grams of calcifediol. This is
USD$0.0533 per milligram.
The base cost of agricultural grade calcifediol is even lower. 1.25% calcifediol (DSM Rovimix Hy-D in 25kg
bags) was worth (according to public import price
records) USD$350/kg in 2020, which is USD$0.028 per milligram.
#99-barc
(Low-key) Oristrell et al. 2021: Barcelona vitamin D3 and calcifediol supplementation study of April 2019 to February 2020
This 2021-07-17 article:
is not particularly significant - but I mention it here
since a naive interpretation of its results might be misleading. This
was an observational study. Ideally a study of the effects of D3 or
calcifediol supplementation would involve randomly chosen supplementing
subjects with those not chosen forming the control group.
There was no real control group and the people considered who were
supplementing D3 or calcifediol were all doing so as part of
prescriptions from their doctors. So this study places
people who are supplementing D3 of their own accord in the control
group.
In the case of those prescribed to take calcifediol, only those who had been tested for creatinine [
WP]
were included. This may be a standard medical test. To some
extent it may indicate that these people with some or many of them were
suffering from from CKD (Chronic Kidney Disease), which is a deadly
condition which greatly increases the risks of bad outcomes with
COVID-19. The control group for those people was a
statistical
selection (propensity score matching [
WP])
of people who were not prescribed either D3 or calcifediol (but who may
nonetheless have been supplementing D3, or less likely calcifediol,
without prescription) where those control subjects were matched as
closely to the subjects in the calcifediol supplementation group. This
is a dodgy process, to say the least.
The calcifediol supplementation group (and the group of individuals
selected for the control group) had an average age of 70, and 83% were
women. This age and sex skew compared to the general population - and
the fact that most or all of the control group, and probably many (due
to propensity score matching) suffered from kidney disease means the
results tell us little or nothing about what would happen if the
general population supplemented with calcifediol.
Furthermore, for the general population, I am not aware of any
advantage of supplementing with calcifediol instead of D3. My sole
interest in calcifediol is as described above - for rapid 25OHD repletion in emergencies.
© 2021 Robin Whittle Daylesford, Victoria, Australia



