The domain name, based on Vitamin D Stops COVID
has turned out to be overly-optimistic, considering new variants of the
virus which are significantly more transmissible than those which were
strongly suppressed in the UK summer of 2020. More
worryingly, researchers have evolved further mutations (without
creating viruses with these mutations) which will be very much more
transmissible than even the currently most transmissible variants: the
independently evolved but otherwise identical South African and
Brazilian variants, which are more transmissible than the recent
"British" variant.
I will retain the domain name for now, but please read the following
update: Vitamin D is vitally important, but I think vaccination and
some masks and social distancing will play an important role in
suppressing COVID-19 (hopefully not outright lockdowns and travel
restrictions) for the next few years and perhaps
indefinitely. If we could suddenly get everyone, in most or
all countries, up to 50 ng/mL
vitamin D blood levels, then this would make a huge difference, but is
probably not enough on its own to render all other control measures
unnecessary. There's no prospect of this occurring in the
next year or so, because the forces of resistance against such
population-scale vitamin D supplementation remain very strong and
because there is not yet sufficient global production capacity to
supply this.
In mid- to late-2020 my sites https://aminotheory.com/cv19/ and https://VitaminDStopsCovid.info
conveyed arguments including my view that the UK 2020 summer lull in
COVID-19 transmission and severity was due primarily to increased solar
UV-B skin exposure raising vitamin D (25OHD blood levels) of most
people in the country sufficiently to, on average:
1 - Strengthen the direct
immune responses to the virus, which are especially weak, on average,
in winter and spring. Low vitamin D causes autocrine (internal)
signaling in immune and other cells to fail: https://vitamindstopscovid.info/02-autocrine/ . So initial defenses were stronger in summer and autumn.
2 - Reduce the hyperinflammatory immune dysregulation (also caused by
autocrine signaling failure in immune cells due to low blood vitamin D
25OHD levels), which causes some people to have severe, debilitating,
lastingly harmful and sometimes deadly, severe COVID-19. Low
vitamin D is the most common, most important, easily correctable cause
of this. See also https://aminotheory.com/cv19/#helminthsgone
for why, without intestinal parasites, and with considerable individual
genetic variation, almost all humans (and domestic dogs and cats) have
systematically overly-strong, self-destructive, inflammatory immune
responses.
3 - Reduce the more thorough spread (with winter-spring low vitamin D
levels) of the virus in the body and so overall symptom severity.
This summer increase in vitamin D levels across the UK population
reduces the total number of viruses shed by each infected person, on
average. I regard this as the most important cause of reduced transmission, with UV-B inactivation of viruses outdoors a second factor.
I surveyed the research on UV-B seasonality (I have not had time to
finalise this on a web page, but if you want a copy of the draft,
please email me) and found strong results showing COVID-19 seasonality
is driven primarily by UV-B radiation changes. There was mixed
research results and unconvincing arguments for the importance of
outdoor high temperatures and/or humidity. (These are of marginal
importance, since in-building and in-vehicle conditions are generally
maintained by heating and air conditioning to be the opposite of summer
and winter extremes - and most close human contact occurs in vehicles
and buildings.)
The high UV-B of summer-autumn has two possible mechanisms for
suppressing COVID-19, influenza etc. transmission and severity:
Firstly, high vitamin D levels, which are pervasive, last for months
and profoundly affect immune responses. Secondly, and I am sure
much less importantly, UV-B inactivates viruses on surfaces and in
aerosols, but only outside buildings and vehicles, since glass blocks
UV-B.
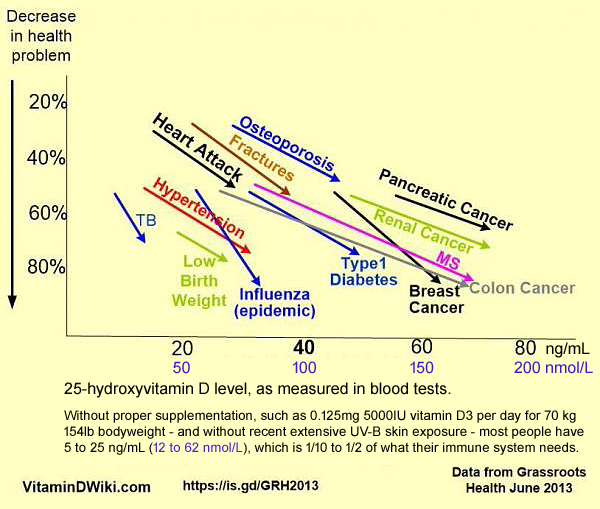
Since, as best we know, UK average 25OHD levels were around 25 ng/mL in summer, I argued that robust (e.g. 0.125mg 5000 IU D3 / day for 70kg adults: https://vitamindstopscovid.info/01-supp/ ) supplementation, which will raise average 25OHD levels to about 50 ng/mL all year round,
and so roughly double the peak summer UK average levels, would suppress
COVID-19 transmission and severity much more substantially than in that
UK summer (as with influenza) to the point of, as I wrote:
. . . there would be no need for lockdowns, social distancing, masks or vaccines.
However, I am no longer confident about this, primarily because of current and likely future mutations in the viral genome which significantly enhance its transmissiblity
- and perhaps (it would not be surprising) the severity of
symptoms. The combination of three mutations in a South
African / Brazilian (the two evolved separately but are the same)
variant is raising most concern in late January 2021:
More detailed, and worrying, molecular-level, details can be found in this French - Israeli preprint (AKA not yet peer reviewed):
#zahradnik
Here are some key points - but remember that I am an electronic
technician trying to understand and summarize bleeding edge
virology:
- The researchers used yeast rather than viruses to
evolve genetic variations on the SARS-CoV-2 spike protein Receptor
Binding Domain (RBD the part of the protein which matches the ACE-2
receptor. This automated process evolves genetic variants far
faster (days weeks and maybe a month or two) than can occur in
SARS-CoV-2 viruses in the wild (months and years).
- They were primarily interested in finding novel
structures which would bind very tightly to the ACE-2 receptor without
upsetting its normal enzymatic function in the body, for the purpose of
introducing such molecules as a drug, in necessarily low
concentrations, to attach to most ACE-2 receptors and so prevent
viruses from attaching to them and so gaining entry into cells.
This is a promising form of antiviral therapy.
- The affinity of a particular RBD for the ACE-2
receptor (here ignoring considerable genetic variation in the ACE-2
structure) is expressed as the concentration required to bind to half
of a population of such receptors. The affinity of the
normal (wild type, before South African / Brazilian mutations) viral
spike protein RBD for the ACE-2 receptor is 1600pM (picomols
concentration). (This is really inverse affinity, since a higher
affinity means a lower concentration of spike proteins with a
particular RBD pattern will bind to 50% of the ACE-2 receptors.)
- The (inverse, to my way of thinking) affinity of the "British" mutation RBD is 455pM, meaning that this RBD has a 1600 / 455 = 3.5 times the affinity of the WT (wild type) original SARS-CoV-2 RBD.
- The South African / Brazilian RBD (with the same, independently evolved, three - Triad, above - mutations) has an (inverse) affinity of 126pM, and so an affinity 1600 / 126 = 12.7 times the affinity
of the WT RBD, which was the main type of SARS-CoV-2 virus present in
the UK in the summer of 2020. The current prevalence of this
strain, and its likely spread throughout the world, is the primary
reason for me thinking that population average 50 ng/mL vitamin D levels
may not "stop" COVID-19, meaning very substantially suppress its
transmission and severity, as much as I anticipated in late 2020.
- The researchers' evolutionary system reliably
produced variants with the same three mutations as the South African /
Brazilian variant. It also produced variants with further
mutations which increased the binding affinity a lot more. Their
best mutation "RBD-62" produces and RBD with an (inverse) affinity of
2.5pM. This RBD has an affinity for the ACE-2 receptor of 1600 /
2.5 = 640 times the affinity of the ordinary, wild-type (not counting British, South African or Brazilian variant) SARS-CoV-2 RBD.
If a soluble form of this RBD was made, it would be a good drug to
reduce SARS-CoV-2 infections, since (depending on its concentration,
which could be quite low) such molecules will bind to most ACE-2
receptors and so prevent viruses from binding to them.
- However . . . this
research, which is perfectly legitimate (and does not involve making
viruses with these genetic variations - they are not allowed to) shows
the specific set of mutations which would give a SARS-CoV-2 virus a very much greater affinity RBD than even the South African / Brazilian variant.
This, and other combinations of mutations they discovered show that there is tremendous scope for the various SARS-CoV-2 strains to evolve still higher affinity RBDs, and so become much more transmissible - since each virus has a higher chance of binding to an ACE-2 receptor.
The 12.7 times higher affinity of the South African / Brazilian RBD
does not translate directly into 12.7 times more transmissibility -
however this might be measured - but the increased transmissibility is
obviously significant, since these variants are spreading faster than
the strains which lack this combination of mutations. The
exact effect of some mutations depends on the presence of others
(epistatic), and may be affected by individual and racial genetic
differences in the structure of the ACE-2 receptor.
SARS-CoV-2 is evolving faster than anticipated.
There's no way of predicting how rapidly still higher affinity strains
will evolve, but it is reasonable to assume that they will evolve in
months or years, not decades.
(Of course, with the information in this article, a person with
suitable equipment and the very worst of intentions could produce a
SARS-CoV-2 virus with these exact mutations and release it.)
Blue boxes on these pages denote quotes from the aforementioned article, with my notes in [square brackets].
This suggests that with the spread of the "British", "Brazilian", and "South African" variants, we project that the Q498R mutation will appear in the future, on top of these mutations. The synergism of Q498R with N501Y and E484K increases ACE2 binding by ~50-fold
relative to WT [ordinary SARS-CoV-2 before the British or South African
/ Brazilian mutations, which have affinities 3.5 and 12.7 times that of
WT].
|
If anyone can find a qualified virologist who can attest that the above
scenario is either exceedingly unlikely, or not cause for a very high
level of alarm, please let me know!
It seems reasonable to assume that these
are the early days of SARS-CoV-2 and so the COVID-19 pandemic, with the
viruses likely to evolve to be very much more transmissible, and likely
cause more serious symptoms, due to being able to spread even when at
much lower concentrations in the body than are required with today's
variants.
- There are other important characteristics of the RBD
part of the spike protein apart from its affinity for the ACE-2
receptor. One is its stability at higher temperatures. The
mutations mentioned in this summary are all no less stable than the WT
RBD.
Another is to what extent the changes in the RBD mean that neutralizing antibodies [WP]
produced in the body by various methods are less likely to bind to a
virus with these altered RBD sections of their spike protein. My
understanding of the text at the top of page 14 is that for this (yet
to evolve in viruses) RBD-62 genetic pattern of RBD, over half of the
tested antibodies (raised by infection and/or vaccination, I guess)
were less able to attach to these spike proteins than they do with the
current strains of SARS-CoV-2. So this particular,
exceedingly high binding affinity RBD genetic pattern, if it evolved in
SARS-CoV-2 viruses, would have significant survival advantages by way
of lower chance of being found by antibodies, in addition to the
immense benefit provides the virus by way of its higher binding ACE-2
binding affinity.
Resistance to proper, robust, population-wide vitamin D3
supplementation remains very strong, in part because many MDs cannot
imagine, and do not care to research, the profound importance of
vitamin D levels being well above the low, to disastrously low (UK
winter) levels they are accustomed to. This is in part due
to lack of understanding of autocrine signaling, and false ideas of
vitamin D acting primarily or solely as a hormone.
It is also hard for MDs to accept that a lot of the chronic diseases
they battle, with great complexity, effort and skill, would be very
much less prevalent if everyone had proper levels of vitamin D and
other nutrients. (A gram of D3 every 22 years is all a 70kg adult
needs to achieve these healthy levels, and a gram costs USD$2.50
ex-factory in 1kg lots.)
Nothing in this update detracts from the importance of raising everyone's 25OHD levels to, on average, 50 ng/mL
(125nmol/L) or so. Its just that I now think the SARS-CoV-2 virus
variants are mutating in ways which mean this disease will be a serious
burden for all people, indefinitely, despite this. However, the
impact of COVID-19 will be very much less if we get the average levels
to 50 ng/mL
than if we fail to do so, and leave them as they are, below 20 ng/mL in
many countries in winter, rising to the mid-20s or perhaps mid-30s if
we are lucky in summer.
It is all the more important to have good vitamin D levels when being vaccinated for COVID-19.
This is well established with influenza vaccines, where stronger immune
responses are elicited in people with higher vitamin D levels:
Effect of 25-hydroxyvitamin D status
on serological response to influenza vaccine in prostate
cancer patients
Manpreet K Chadha, Marwan Fakih, Josephia Muindi, Lili Tian,
Terry Mashtare, Candace S Johnson, Donald Trump
Prostate 2010-09-01
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4718551/
|
Baseline Serum Vitamin A and D Levels
Determine Benefit of Oral Vitamin A&D Supplements to
Humoral Immune Responses Following Pediatric Influenza
Vaccination
Nehali Patel et al. Viruses 2019-09-25
https://www.mdpi.com/1999-4915/11/10/907
|
Vaccines vary in their effectiveness and risks of serious
ill-effects. It is far too early to tell to what degree any one
vaccine will really protect against COVID-19 infection, for all the
strains of the virus in circulation now or in the future.
We don't know how long vaccine-induced immunity will last, or to what
degree it is specific to particular strains of the virus. There
are concerns about lack of testing in frail older folks, with
potentially poorer immune responses and higher risks of serious
ill-effects, such as Bells Palsy: https://covid.us.org/2020/12/23/is-there-a-risk-of-bells-palsy-with-mrna-covid-19-vaccines/ .
The popular vision, driven by popular hope and the statements of
politicians, is that once most people are vaccinated, life can return
to normal. There is no prospect of this being true, since
the viral strains will continue to mutate, since immunity from vaccines
and prior infections will fade, since vaccine effectiveness will vary
with numerous personal characteristics - including especially age,
obesity and low vitamin D levels.
Close to the equator, some countries are doing pretty well. But
people there tend to have dark skin and, wisely, avoid direct sunlight
- so vitamin D levels can still be lower than required for proper
immune function.
Far from the equator, seasonal variation in UV-B skin exposure will
drive very strong seasonal patterns in COVID-19 transmission and
severity.
Even if more than half the population of many countries are vaccinated
by the end of 2021, the virus will still be transmitted, with
increasing likelihood of variants which infect people with immunity to
prior forms of the virus, either through prior infection or
vaccine-induced immunity. The vaccination programs put the virus
under selection pressure to evolve in ways which avoid being detected
by the immunity raised by current vaccines. So this will be a
global cat and mouse game between the virus variants and the vaccine
manufacturers.
Moderate or severe COVID-19 can cause very long lasting problems -
probably permanent loss of capacity - for quite a high proportion of
people. It is a serious disease, and people who minimise
its importance, such as by quoting average ages of those killed by, or
with, COVID-19, are avoiding the impact it has on many people in their
twenties to fifties. They are also avoiding the impact it has on
children by triggering Kawasaki disease or Multisystem Inflammatory
Syndrome: https://aminotheory.com/cv19/#2015-Stagi .
Even if governments decided to have their entire populations supplement
D3 properly tomorrow, world production of pharma grade D3 would soon be
overwhelmed if more than a few tens of millions of people adopted
this. D3 factories take years to build by ordinary means -
and those running now operate 24 hours a day. Governments
should work together globally with an urgency normally only found in
times of war to build new pharma-grade D3 factories. In the
meantime, we should direct some of the much greater animal feed grade
D3 production for humans.
Omega 3 fatty acids should also be recommended to the population for
substantial daily supplementation. There are numerous health
reasons for this, and now must urgently regarding COVID-19: Asher et
al. https://www.plefa.com/article/S0952-3278(21)00013-2/
The trouble is people need grams of fish or algae oil a day, when they
only need, on average 1/8000 of a gram of D3. I can't imagine
how global production could be ramped up to a few grams per day per
person, which is what everyone needs. B vitamins: the same story
but the quantities are smaller than for omega-3 fatty acids, so
production could be ramped up. But all these are far more
expensive than vitamin D, and vitamin D is surely the most important
nutritional deficiency which needs to be fixed for reasons of general
health and COVID-19 in particular. Zinc - best to take 25mg or so
a day as chelate. Some people are sensitive to excess zinc, so
more than this may be a problem.
In the coming months or years it seems likely that SARS-CoV-2 variants
will become very much more transmissible than they are today.
Then, perhaps, vaccines would not be able to produce the very high
concentrations of antibodies, to the various strains, which would be
required to either prevent infection or seriously reduce the risk of
severe symptoms.
This would leave us with the following options for avoiding severe symptoms, and reducing transmission to some extent:
- High, continual, doses of antiviral drugs for a
substantial fraction, or most, of the population. This would be
extraordinarily expensive, difficult to ramp up to this massive scale,
and would surely cause significant ill-effects.
There are quite a number of possible antiviral drugs and combinations
of nutrient which directly reduce viral replication, so these should
not be ruled out for vulnerable people, but this is not a solution to
the whole problem.
- More mask, social distancing and lockdowns - we are
already at our limit with these and the costs are extraordinarily
high. This is no way to live into the indefinite future.
- Nutritional supplements to boost direct antiviral
immune function and, most importantly, to greatly reduce the tendency
of many or most people to having dysregulated, hyper-inflammatory,
immune responses to SARS-CoV-2, influenza etc.
First and foremost this means population-scale vitamin D supplementation to attain average 25OHD levels of around 50 ng/mL .
The costs and practicalities of other supplements are more challenging
than D3 supplementation. Boron is likely to be helpful, but
it needs to be taken every day and many people do not recognise it as a
nutrient. Borax is banned in the EU, for no good
reason. Vitamin C is also a daily intake
nutrient. Various B vitamins are surely important.
Zinc needs to be taken once a day, and some people are sensitive to
higher levels - but as far as I know 25mg a day is OK for adults.
(Zinc and other minerals have some interactions at the time of
ingestion, so it can be complex to schedule when to have such
nutrients. Also, zinc as oxide is not as bioavailable as
chelate.)
Selenium may help too.
Omega 3 fatty acids are surely beneficial but these are bulky and
expensive, and it takes months, as far as I know, to alter the omega-3
to omega-6 ratio in the body's overall circulating, stored and
in-membrane fatty acid makeup.
In short, very much increased SARS-CoV-2 transmissibility may make
vitamin D and other nutrients the only long-term sustainable way we can
cope with these viruses. All the above nutritional
supplements have broad, profound, health benefits, and are worth doing
anyway even if there was no COVID-19 pandemic.
|